
Modern Mental Status Exam – Its Structure and Historical Roots
Abstract
The mental status exam remains the core element of psychiatric assessment, forming the basis for our diagnoses and documentation of the patient’s presentation at a moment in time. This tool, and to some degree our entire field, remains rooted in a lexicon which was developed over a century ago; terms which have served the field well, but are now largely out of step with a modern understanding of the brain as a dynamic information-processing and energy-regulating system. This disconnect represents more than a benign anachronism, it creates a barrier between the bench and bedside, restraining our field from the incredible progress seen in other branches of medicine since the mid-19th century. It also leaves our field poorly prepared for a future, in which we will be called to assess not only a single mind, but extended minds in combination with technology. Here I argue for a functional mental status exam, a first-principles-oriented approach to assessing the integrity of a dynamic nervous system, and suggest a few guideposts to frame this new approach to patient evaluation.
The mental status exam (MSE) is the physical exam of psychiatry and forms the bedrock of our assessment. At its core, it represents a written description of our interaction with the patient based on both direct observation and interview responses. As with other branches of medicine, this exam is meant to capture information of relevance to diagnostic classification, with the aim of better understanding how a specific patients’ symptoms align with the historical experience of our field. In so doing, we can develop better predictive models (both diagnostic and prognostic) and recommend treatments which may help change the trajectory of that prediction. While other branches of medicine have gradually supplemented or swapped direct patient observation with technological modes of assessment, for psychiatry, we remain largely reliant on our analog MSE.
The exam as it is practiced, and taught today, looks highly reminiscent of the descriptive psychopathology approach used in the 19th century, using terms defined nearly 200 years ago [Berrios, 2010]. Indeed, while the exact wording and structure have changed, the core MSE elements assessing perception, thought, emotion and volition are highly preserved when one compares our modern texts with those of the past two centuries. To this has been appended a more detailed assessment of cognition (sometimes called the “neurological MSE”) which is an homage to the work of neuropsychologists and cognitive neurologists over the past 50-100 years [Mesulam, 2000]. Thus, today’s mental status exam would be completely recognizable to historical giants of our field, but for some assistance in interpreting our proclivity toward abbreviations (SI, TP, etc…).
Do we need more “bench” or better “bedside”?
The issue with the MSE is not simply that it is old; there are a number of historically defined concepts across all fields of medicine which have stood the test of time. Nor is it in the use of a subjective and cross-sectional set of observations; there remains much in medicine which relies on observer-dependent descriptions of a singular observation (e.g. edema severity, murmur grading, or motor strength). The issue is that in other areas of medicine these observations are markers of pathology connected back to an understanding of the underlying functional physiology. Thus, even seemingly disconnected and subjective physical exam findings (e.g., course rales at the lung bases, elevated jugular venous pressure, and pitting edema at the ankles) can all be connected to underlying physiology and its known failure mode (in this case, related to the heart) and refined by technological assessment (echocardiography). This is not true for our field. Our exam findings remain a loosely connected set of comments without a clear connection to the underlying functional neurophysiology.
This divide is not of course a new concern, we have never had clear one-to-one mapping between symptoms and their genesis in the brain. Most have argued that we need a better understanding of the brain to close this gap, an argument which has fueled incredible neuroscience research for the better part of 50 years. But what if the issue is not more focus on the bench, but rather better description at the bedside?
Our brain, and its extensions into central, peripheral and autonomic nervous systems, serves two core functions: to understand and control [Parr et al., 2022]. It carries out these predictive and regulatory functions both within our bodies (interoceptive) and in the environment (exteroceptive). People who are better able to use energy extracted from food to predict and engage in the world, including predicting and engaging with others, are more likely to survive.
Our understanding of the predictive and regulatory functions carried out by our nervous systems is actually quite robust. And the revealed neurophysiology is truly extraordinary. The way in which we utilize and preserve energy through finely tuned sleep-wake or appetitive-cycles [Eban-Rothschild et al., 2018]. The energy-preserving role of the basal ganglia, in the creation of motor and cognitive scripts [Huey et al, 2008]. The function of the hippocampus to time travel, allowing us to both recall prior events and imagine unfolding futures [Schacter et a, 2007]. In these and so many other myriad ways, our brains allow us to regulate ourselves and interpret the dynamic and chaotic states of nature. But, each of these functions can fail, and these “failure modes” form the basis for what we call mental illness.
It is not a need for more neuroscientific understanding which is holding our field back. It is that our description of what we see at the bedside has fallen out of step with this understanding. It is very hard to draw a line from our static, loosely organized, set of subjective descriptors to the neurophysiology (or pathophysiology) which is at their root. Our present MSE does not capture the breakdown of the core predictive and regulatory functions which can go amiss. Nor does it reflect the dynamism and interconnectivity of these functions.
These limitations are important for three primary reasons:
Malalignment of our clinical descriptors and our extant neuroscience research precludes meaningful combinations which could advance the field. Our understanding will stagnate
Without meaningful connection back to neurophysiology, our explanations will lose resonance with the people experiencing these symptoms. As confidence in (big-P) Psychiatry as an explanatory model wanes, people will turn to other framing approaches. This is true for all of Medicine, but perhaps a greater threat for our field, given lower barriers to entry.
Without better descriptions of the clinical manifestations of functional impairment and its connection to known physiology, our field will be incredibly ill-prepared as people increasingly offload these predictive and regulatory functions to others or to technology. Our current MSE assumes bounded, isolated, minds in a vacuum, and yet each of us is dynamically interconnected with our tools and each other. The integrity of these connections can also fail…our exam at present is not capable of capturing that.
A Proposed Functional Mental Status Exam (fMSE)
While there is no universal standard for the traditional MSE, many document it using the acronym ABSEPTIC (Appearance, Behavior, Speech, Emotion, Perception, Thought, Insight and Cognition). Typically, “emotion” includes a statement of the patient’s mood and a static description of their affect. The section on “thought” generally includes thought processes (e.g, “linear and goal directed”) and thought content, including any suicidal, homicidal or delusional ideation. Sometimes Judgement is included with Insight and often the Cognition section includes a brief bedside exam, or structured results from a tool like the Montreal Cognitive Assessment.
Nervous system axes: Interoceptive and Exteroceptive
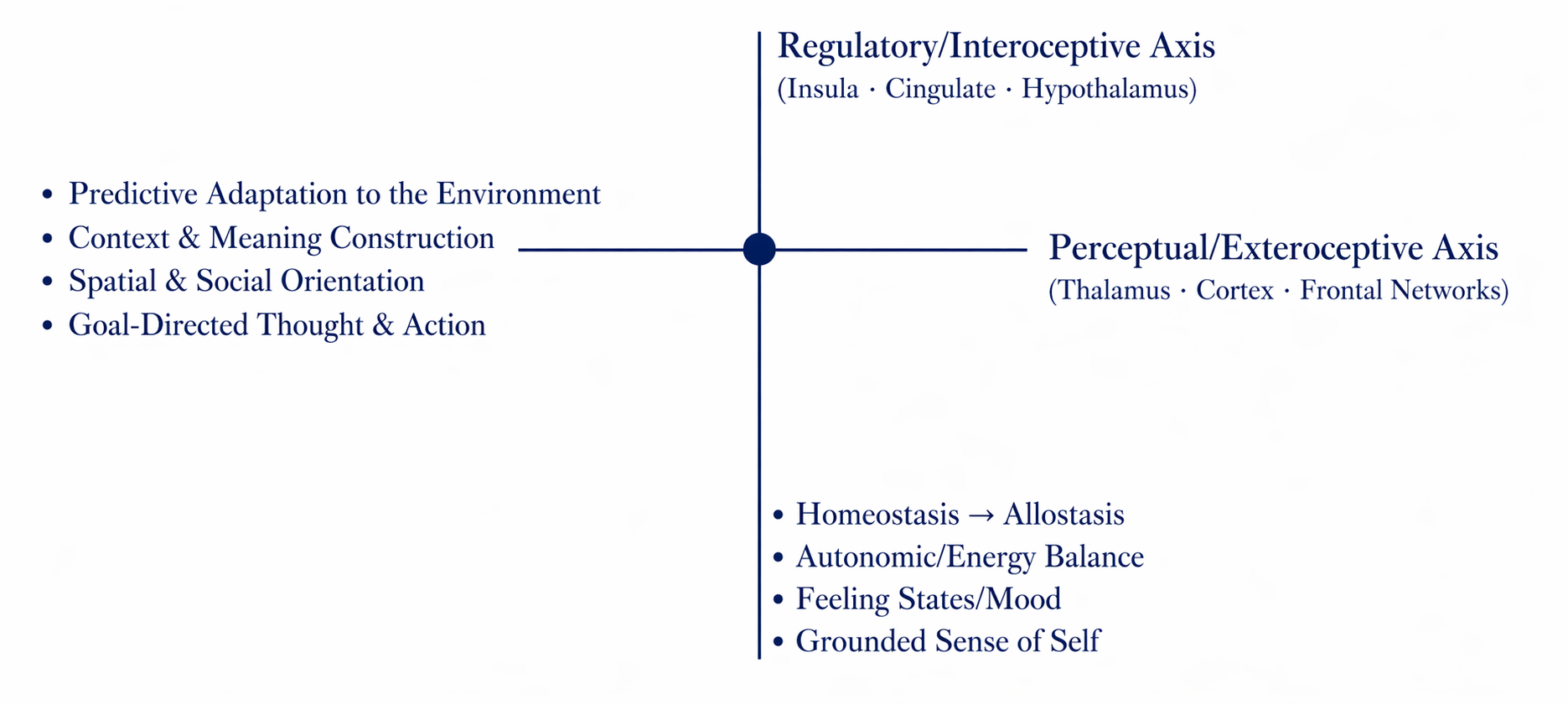
The framework of my proposed fMSE shifts from a collection of findings organized by an acronym to a model oriented around first principles, assessing the integrity of the two fundamental functions of our mental infrastructure: regulation and prediction. It does this using the two primary central nervous system axes, interoceptive and exteroceptive, and their intersection (Image on right).
With each axis one can consider various subdomains which map to familiar functions: for example, within the Interoceptive Axis we can assess Energy and Drive Modulation, a subdomain comprising sleep-wake cycles, appetitive cycles, activity patterns, and motivation.
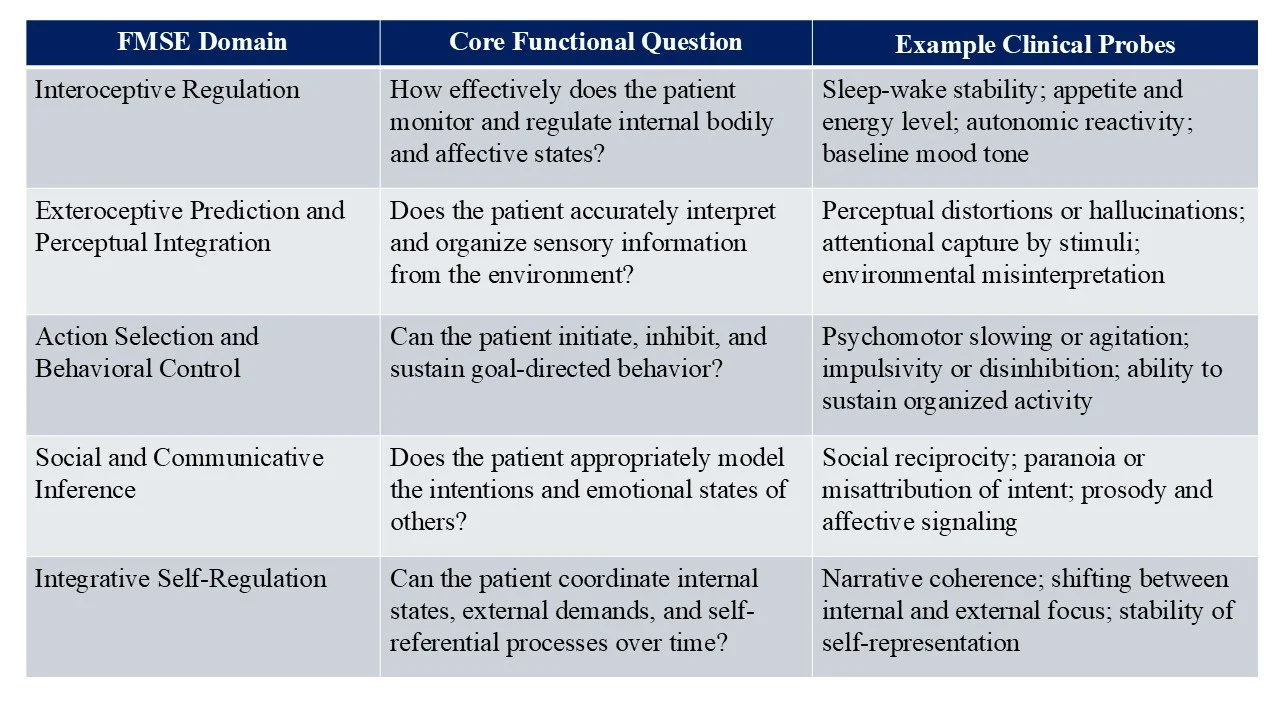
General framework, including key domains and sample clinical probes
There is no new interview required. One need not completely shift the way in which we elicit symptoms and observe behaviors. But it does require a bit of conceptual remapping. Practically it requires reshaping our templates, so that (for example) questions about sleep and food intake are captured here alongside descriptions of thought process. It also requires splitting up concepts like “mood and affect”, which rather than simple one-word descriptors are actually complex constructs which reflect internal regulation, integration of that internal state with external expression, and bi-direction interaction with the environment. The language also needs to shift to convey the dynamism of these functions both over time and in the interaction with the interviewer and broader environment.
Thus:
Mood: “Good”. Affect: Euthymic
Becomes:
Patient’s stated mood at present is “good”. Affective baseline is generally congruent with this - neutral to slightly positive as reflected in good eye contact, upright posture, and vocal tone. Affect demonstrates preserved dynamic range with appropriate response to both the nature of conversation and interpersonal cues. Occasionally receives affective reassurance from partner (at bedside) who makes statements like “it’ll be ok” and gently strokes her hair. With emotionally evocative content, there is rapid recovery.
Relationship to Psychiatric Diagnosis
The fMSE itself is not a diagnostic tool. It is a set of observations reflecting the integrity of the functions of the brain, and as such it begins from a normative frame, rather than a pathological frame. While one can use the fMSE to create DSM-valid diagnoses it is meant to better align symptoms with disrupted function, rather than statistical categorizations. In so doing, it is actually easier to teach and more resonant with patient’s experience of their illness.
On its face, there are similarities here between the fMSE and recent initiatives such as the Research Domain Criteria (RDoC) framework [Insel et al, 2010], in that both are attempting to match aspects of patient behavior to an understanding of the functional organization of the brain. The fMSE is not a research classification system, but is rather a structured clinical exam designed for practical use. Nor is the fMSE oriented around specific neural circuits, but rather around dynamic functions of the brain in a manner agnostic to the neurocircuitry which generates it. In a sense, the fMSE could be construed as a clinical counterpart to these domain-based research approaches, though this would require some mapping to more formally correlate them.
Future Directions
For the fMSE to move from concept to practical tool, significant work would need to occur. Standardization of bedside probes, assessment of inter-rater agreement, correlation with clinical utility, all at minimum. Linkage to behavioral or physiological monitoring would also be useful, especially if we construe this as a stronger form of digital phenotyping. And inclusion of assessment of the extended system of the mental state, that is the integrity of the connections between the patient and their close supports (human and technological), would help move this assessment toward a more flexible model inclusive of these extensions. By presenting this now, even in this initial phase, my aim is to encourage a dialog which would allow for these refinements.
Our assessment still relies on an exam largely developed in a different conceptual era. And while human nature has not changed, our understanding of the physiology underpinning that nature has. Advances in neuroscience emphasize the incredible predictive and regulatory capacity of our nervous system, and how it can be scaffolded by others or technology. Developing a clinical assessment in line with these principles is a key next step in advancing our field and better caring for the patients who need our assistance.
-
Berrios G.E. (2010). The History of Mental Symptoms: Descriptive Psychopathology Since the 19th Century. Cambridge University Press.
Eban-Rothschild A, Appelbaum L, and de Lecea L (2018). Neuronal Mechanisms for Sleep/Wake Regulation and Modulatory Drive. Neuropsychopharmacology 43: 937-952.
Huey ED, Zahn R, Krueger F, Moll J, Kapogiannis, D, Wassermann EM, and Grafman J (2008). A psychological and neuroanatomical model of obsessive-compulsive disorder. J Neuropsychiatry Clin Neurosci 20(4):390–408.
Insel T, Cuthbert B, Garvey M, Heinssen R, Pine DS, Quinn K, Sanislow C, & Wang P (2010). Research domain criteria (RDoC): toward a new classification framework for research on mental disorders. Am J Psychiatry, 167(7), 748–751
Mesulam M-M (2000). Principles of Behavioral and Cognitive Neurology, 2nd Edition. Oxford University Press.
Parr T, Pezzulo G, and Friston KJ (2022). Active Inference: The Free Energy Principle in Mind, Brain and Behavior. MIT Press, Cambridge, MA
Schacter, D. L., Addis, D. R. & Buckner, R. L. (2007). Remembering the past to imagine the future: the prospective brain. Nat. Rev. Neurosci. 8, 657–661.